


Assessing Risk and Protective Factors in Clinical and Judicial Child-to-Parent Violence Cases
[La evaluaci├│n de factores de riesgo y de protecci├│n en casos cl├şnicos y judiciales de violencia filio-parental]
Ismael Loinaz1,a and Ava Ma de Sousa2,a
1University of Barcelona, Spain; 2University of Toronto, Canada
https://doi.org/10.5093/ejpalc2020a5
Received 6 March 2019, Accepted 7 November 2019
Abstract
Child-to-parent violence takes different forms (physical, psychological or economic) and can be addressed in the judicial system or in clinical practice. The current paper compares 61 clinical and 30 judicialized cases that were evaluated using the Child-to-Parent Violence Risk assessment tool (CPVR). Results showed a higher prevalence of risk factors in the judicialsample. This group of aggressors had worse profiles of violence (bidirectionality of the parent/child violence, violenceother than CPV, and more CPV complaints), more psychological issues (low frustration tolerance, little anger management,narcissism, and violent attitudes) and, most notably, more dysfunctional families (violence between parents, cohabitationproblems, inversion of the hierarchy, non-violent conflicts, and even criminal history of the parents). Logistic regressionshowed that narcissism, attitudes justifying violence, violence between parents, and problems of parents themselves(such mental disorders or drug abuse) allowed for correct classification of 89.4% of cases. Total CPVR scores differedbetween groups (25.8 vs. 14.2), and classification was good for both type of group (AUC = .830) and injuries to mother (AUC= .764). A cut-off score between 22 and 23 showed the best results in prediction of group and injuries to mother. Utility ofthe CPVR, and next steps in its development are discussed.
Resumen
La Violencia Filio-Parental (VFP) puede manifestarse de distintas formas (física, psicológica o económica) y su abordaje puede hacerse desde el sistema judicial o desde la práctica clínica. El presente estudio compara 61 casos clínicos (no judicializados) y 30 judicializados que fueron evaluados con la Guía para la Valoración del Riesgo de Violencia Filio-Parental (RVFP).Los resultados mostraron una mayor prevalencia de los factores de riesgo en la muestra judicial, con un perfil de violenciapeor (más bidireccionalidad, más violencia distinta a la VFP y más denuncias por VFP), más complicaciones psicológicas enlos agresores (baja tolerancia a la frustración, poco control de la ira, narcisismo y actitudes violentas) y, en especial, un perfilfamiliar más disfuncional (violencia entre los padres, problemas de convivencia, inversión de jerarquía, conflictos e inclusoantecedentes delictivos en los padres). Una regresión logística puso de manifiesto que el narcisismo, las actitudes que justifican la violencia, la violencia entre los progenitores y los problemas de los padres (como trastorno mental o abuso de drogas)permitían clasificar correctamente al 89.4% de los casos. El grupo midió diferencias en la puntuación en la Guía RVFP (25.8vs. 14.2) y la clasificación fue buena para el tipo de grupo (AUC = .830) y lesiones a la madre (AUC = .764). Un punto de corteentre 22 y 23 mostró los mejores resultados en la predicción del grupo y las lesiones a la madre. Se discute la utilidad de laRVFP y los siguientes pasos en su desarrollo.
Keywords
Child-to-parent violence, Violence risk assessment, Clinical context, Judicial contextPalabras clave
Violencia filio-parental, Evaluaci├│n del riesgo de violencia, Contexto cl├şnico, Contexto judicialCite this article as: Loinaz, I. and Sousa, A. M. D. (2019). Assessing Risk and Protective Factors in Clinical and Judicial Child-to-Parent Violence Cases. The European Journal of Psychology Applied to Legal Context, 12(1), 43 - 51. https://doi.org/10.5093/ejpalc2020a5
iloinaz@ub.edu Correspondence: iloinaz@ub.edu (I. Loinaz).Child-to-parent violence (CPV) is a subtype of family or domestic violence, also referred to as “parental abuse”, “youth violence toward parents”, or “adolescent aggression towards parents”. In fact, the lack of agreement with respect to operational definitions has been pointed out in previous research (Kennedy, Edmonds, Dann, & Burnett, 2010). In 2017, the Spanish Society for the Study of Child-to-Parent Violence (SEVIFIP) published a proposal of an agreed-upon definition (Pereira et al., 2017) based on available works: Repeated behavior of physical, psychological (verbal or nonverbal) or economic violence, directed toward the parents or caregivers. Excluded are one-off aggressions that occur in a state of diminished consciousness disappearing upon recovery (intoxications, withdrawal syndromes, delirious states or hallucinations), those caused by (transient or stable) psychological disorders (autism and severe mental deficiency) and parricide without history of previous aggressions (p. 220). Different forms of domestic/family violence, like CPV and elder abuse were neglected in the literature until some years ago (Walsh & Krienert, 2007). In recent years, interest in this area has grown considerably and, therefore, statistics have become available. Estimates of CPV prevalence are difficult to calculate, given that most cases do not involve an arrest or police record. Kennedy et al. (2010) explained how CPV may not appear to be a significant problem compared to other types of violence, but there is need for consideration of the fact that such violence is often kept private (since parents tend to be reluctant to report their children). Because the issue involves a son/daughter causing harm to their caretaker, who is meant to be in charge, there is often stigma and blame attached to the victims. Moreover, sometimes the parent is seen as being responsible for the situation (Walsh & Krienert, 2007), increasing felt sense of shame. This leads to a reluctance to report until the problem becomes unbearable, or a lack of reporting altogether, limiting the data on what is known about CPV. International rates on CPV are highly variable, making it difficult to determine the extent of this type of violence (O’Hara, Duchschere, Beck, & Lawrence, 2017; Simmons, McEwan, Purcell, & Ogloff, 2018). Global estimates range from 5 to18% for physical forms of CPV between different samples (Calvete, Orue, & Sampedro, 2011; Holt, 2012; Kennair & Mellor, 2007; Pagani et al., 2009). Psychological violence is much more common, making up over 90% of CPV cases if less severe forms are included. The more restrictive the definition and the more severe the behaviour, the less prevalent it becomes. Analysing specific samples of CPV offenders, clinical samples are more similar to the general population regarding their violence (i.e., Calvete, Orue, & Gámez-Guadix, 2013; Nock & Kazdin, 2002) and forensic/judicial samples have the highest prevalence of physical and psychological violence (i.e., Ibabe, Arnoso, & Elgorriaga, 2014a). In Spain, for instance, there are an average of 4,600 cases per year reported in the judicial system since 2007 according to State Attorney’s Office statistics (Loinaz, Andrés-Pueyo, & Pereira, 2017), representing cases that have reached breaking points, the final step in this type of violence. Research on CPV: What do We Know? CPV appears to most commonly occur during the adolescence of the perpetrator, though it is not limited to minors (González-Álvarez, Gesteira, Fernández-Arias, & García-Vera, 2010; Holt, 2016; Moulds, Day, Mildred, Miller, & Casey, 2016; Walsh & Krienert, 2009). Research into CPV has shown conflicting information on gender of the perpetrator, although much research suggests there to be more male perpetrators (Ibabe, et al., 2014a; Nock & Kazdin, 2002; Routt & Anderson, 2011; Walsh & Krienert, 2007). Yet, these numbers do not represent every instance of CPV, but rather only those that are reported. Thus, many social factors and pressures influence the prevalence rates accessible to researchers, such as possible shame from fathers feeling a subjective loss of control (Walsh & Krienert, 2007), as well as the perception that a boy is more of a serious threat than a girl (Ibabe & Jaureguizar, 2010). There is thus a need for further research before most common gender of perpetrator can be determined. Among offenders, girls tend to commit more psychological abuse (e.g., Beckmann, Bergmann, Fischer, & Mößle, in press; Rosado, Rico, & Cantón-Cortés, 2017), while boys tend to physically assault more than girls, both in the clinical and judicial context (Boxer et al., 2009; Routt & Anderson, 2011). Some studies have analyzed specific risk factors of CPV (Beckmann et al., in press; Ibabe, Jaureguizar, & Bentler, 2013; Pagani et al., 2004, 2009), and certain factors have been found repeatedly among offenders and their families. Perpetrators often face mental health issues, such as depression, ADHD or antisocial personality disorders (Castañeda, Garrido-Fernández, & Lanzarote, 2012; Coogan, 2014; Ibabe & Jaureguizar, 2010; Routt & Anderson, 2011). Compared to young offenders who had committed crimes other than CPV, CPV offenders were found to have worse psychopathological profiles, with 30% having received a clinical diagnosis (most commonly ADHD), while no clinical diagnoses were found in the non CPV sample (Contreras & Cano, 2015). Other individual factors related to the perpetrator such as lower self-esteem (Calvete et al., 2011; Ibabe et al., 2014a; Ibabe, Arnoso, & Elgorriaga, 2014b; Pereira & Bertino, 2010), lower empathy (Castañeda et al., 2012; Ibabe & Jaureguizar, 2010), higher impulsivity (Calvete et al., 2011; Ibabe et al., 2014a; Pereira & Bertino, 2010), and lower frustration tolerance (Kennair & Mellor, 2007; Nock & Kazdin, 2002) have been linked to CPV offenders, both compared to youth of normal profiles as well as young offenders. Tied in with mental health and individual profile characteristics are issues of substance abuse (Calvete et al., 2011; Castañeda et al., 2012; Ibabe et al., 2013; Routt & Anderson, 2011), which are found at even higher rates in CPV cases compared to other young offenders (Ibabe & Jaureguizar, 2010; Ibabe, Jaureguizar, & Díaz, 2009). External risk factors of CPV are behavioral and academic problems in school (González-Álvarez et al., 2010; Ibabe & Jaureguizar, 2010). Within the context of school also lies the issue of bullying victimization, which research suggests might account for origins of aggressive behavior (Cottrell & Monk, 2004). This idea of aggression leading to further aggression is an important line of discussion in CPV research. Though CPV offenders seem to display more aggression outside the home than other young offenders (Ibabe et al., 2014a), the cycle of violence is especially important in the context of the home. While CPV perpetrators are often referred to as offenders, and their parents as victims, sometimes the roles are also reversed, and the child can him/herself be the victim of violence at the hands of their parents. This bidirectionality has been noted as a possible explanatory factor (Del Hoyo-Bilbao, Gámez-Guadix, & Calvete, 2018). Indeed, direct exposure to violence in the home, as well as indirect exposure (witnessing violence between parents or between other family members) have been correlated with CPV (Boxer, Gullan, & Mahoney, 2009; Contreras & Cano, 2016; Gamez-Guadix, Jaureguizar, Almendros, & Carrobles, 2012; Routt & Anderson, 2011). A recent meta-analytic review (Gallego, Novo, Fariña, & Arce, 2019) found that the risk of developing CPV among children victimized by their parents increased 71% as compared to non-victimized children. This supports the idea that both direct victimization of children as well as exposure to vicarious violence are significant predictors of CPV. Nevertheless, a comparison between CPV offenders and non-CPV youth offenders showed that while both were more likely than the average child to be exposed to violence in the home, the prevalence of CPV offenders who witnessed violence in the home was even greater than in non-CPV offenders, demonstrating the strong influence of family violence on CPV cases (Contreras & Cano, 2016). Problems in the home relating to CPV go beyond family violence. Problematic education styles often occur, with the parent unable to establish clear norms (Aroca, Miró, & Bellver, 2013; Castañeda et al., 2012). Possibly related to this issue of instability is the composition of families wherein this type of violence occurs. A disproportionate amount of single-parent families faces these issues (Ibabe & Jaureguizar, 2010), and Contreras and Cano’s (2014a) found that CPV offenders were more likely than other young offenders to come from single parent homes. The correlation between family composition and CPV might also be mediated by the lack of support and, as mentioned before, instability sometimes accompanying these situations. Indeed, some studies have found no correlation between family composition and CPV vulnerability (Beckmann et al., in press; Pagani et al., 2004). There are conflicting reports as to the link between the socio-economic status of the family and CPV. While some studies suggest lower socio-economic status families to be more vulnerable (Condry & Miles, 2014; Cottrell & Monk, 2004), others find no correlation (Calvete et al., 2011), while others still see the opposite effect (Kennair & Mellor, 2007). In the CPV literature, few studies have analyzed protective factors. Those that have have noted the importance of self-control of the child, paternal warmth (Beckmann et al., in press), and parental affection and communication (Calvete, Gámez-Guadix, & Orue, 2014; Ibabe & Bentler, 2016). There are other general protective factors for youth offences, some shared with adult violence cases and others more specific to youth offenders, such as parental, peer, and community support, which are included in assessment tools such SAPROF-YV (see de Vries Robbé & Willis, 2017), a structured guide for the assessment of protective factors (during violence risk assessment) in youth. The Assessment of CPV Holt (2012), in a critical review of research on CPV, argued that the field is a long way from understanding the relevance of specific risk factors in particular populations and from understanding whether treatment programs, or specific elements of treatment, facilitate changes in violence patterns. Recently, there have been some proposals of new assessment tools for CPV, such as the Child-to-Mother Violence Scale (Edenborough, Wilkes, Jackson, & Mannix, 2011), designed to capture the prevalence, experience, and nature of child-to-mother violence, and the Intra-family Violence Scale (Ibabe et al., 2013), with nine items designed to assess the presence of violence toward parents, parent-to-child violence and between-parent violence. Other recent tools are the Child-to-Parent Aggression Questionnaire (Calvete et al., 2016), with a revised version including reasons for the abuse (Calvete & Orue, 2016), and the Child-to-Parent Violence Questionnaire (Contreras, Bustos-Navarrete, & Cano-Lozano, 2019), focused on type and prevalence of violence committed, as well as self-reported reasons for the acts by the aggressors. To our knowledge, the one used in the present research is the only specific violence risk assessment tool for CPV cases (see Loinaz et al., 2017). Moreover, youth violence is commonly analyzed as a homogeneous problem and risk assessment tools for youth are mostly designed for antisocial offenders or common crimes. CPV has not yet been looked at from this methodological viewpoint, and it therefore demands the use of a tool better tailored to this specific type of violence and surrounding circumstances. Current Work The present work sought to compare two samples of youth implicated in CPV (clinical and judicial), applying a recently developed violence risk assessment tool. The main question was to examine what distinguishes these two populations according to risk factors, pushing certain parents choose to have their children treated in a clinical context, while others report the offenses suffered to the justice system. It was hypothesized that families who chose clinical recourse would be less problematic, more involved with the child in question, and possibly have suffered less serious violence. It was expected, on the other hand, that judicial cases would be more serious (perhaps even including a history of other kinds of crime) or would have offenders coming from families with fewer resources, more legal problems, or who were less involved in their child’s treatment. Sample The sample was composed of 91 cases, 67% coming from clinical centers (11 from Euskarri, and 49 from Amalgama7) and 33% coming from judicial contexts/measures (22 from the SMAT of Barcelona, and 9 from Fundación Pioneros [Pioneers Foundation]). Those in clinical contexts were there in a private capacity, paying for service (without a judicial statement requiring compulsory treatment). Those in judicial contexts were there to be assessed for a CPV crime or doing a program serving a sentence (either court ordered or recommended). The average age at the time of assessment was 17.07 (SD = 2.40, range = 13-28), 61.5% (n = 56) were men, and 93.4% (n = 85) were of Spanish nationality. Regarding the comparison of the groups, there were significantly, χ2(1, 91) = 6.27, p = .012, more girls in the clinical group (56.7% vs. 29.5%). The clinical group was also significantly older, t(87) = 2.43, p = .003, than the judicial group: 17.50 years of age (SD = 2.76) vs. 16.23 years (SD = 1.07). There were no significant differences in nationality, with a majority of Spanish participants in both samples (91.8% in clinical sample, and 96.7% in the judicial sample). Materials The version 2.1 of the Child-to-Parent Violence Risk assessment tool (CPVR; RVFP in its original name) was used, which has been in the process of validation since 2014 (Loinaz et al., 2017). The tool was created following current international standards (see Douglas et al., 2014), consisting of three main steps: 1) the review of studies and available tools from which a list of relevant risk factors was obtained; 2) gathering professional feedback regarding risk factors and the tool proposal; and 3) a pilot application before the publication of the instrument. The tool is composed of 24 risk factors organized into four blocks (type of violence, psychological charactersitics of the perpetrator, adaptation of the perpetrator, and family factors), and six protective factors (see Table 1). These factors are coded as present (Yes), partially present (?) or absent (No) for the present time (during the last year) and for the past. Moreover, the risk assessment tool includes a first section in the worksheet with more than 20 possible risk factors (i.e., single-parent family, adoption, academic situation, members of the family, immigration, parents’ criminal histories, death of a close family member, cause of the assessment, prior convictions, type of violence, type of victim, and so on). Table 1 Prevalence of Risk and Protective Factors 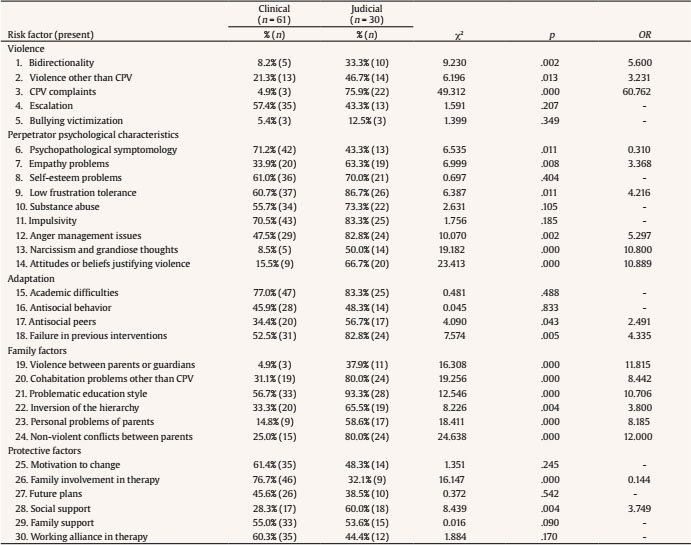 Note. 1Although the item includes both parents, in this sample only fathers had criminal records. Procedure All the cases were directly assessed by professionals belonging to each center and were statistically analyzed with anonymity maintained. The assessments were part of the usual procedure of each service, therefore not influencing the analyzed cases in any way. For the samples of Amalgama7 and SMAT, the risk assessment tool was coded from case files by forensic psychology Master’s students (see Coding section). In the case of Euskarri and Pioneros, professionals of the centers assessed the cases and also coded the tool. The cases were added together and put into a database as part of the validation process of the instrument. Coding The coding of the tool was carried out following a detailed guide. This included the definitions of the items, a worksheet with a summarized explanation of when a factor should be considered present, and a worksheet in a Word file in which the presence of the factors both past and present were recorded, with the decision explained with transcription of information from records (useful information to verify the reliability of the coding). The reliability of the coding of each item of the CPVR regarding available file information was analyzed with true kappa. Researchers (not clinicians) were trained with other cases that were not part of the present study, discussing discrepancies in coding until consensus was reached. True kappa is calculated like Cohen’s kappa but verifying the correspondence between the sources used for coding (Vilariño, Arce, & Fariña, 2013). The results of true kappa are interpreted as weak (< .60), high (> .61-< .81) or very high (≥ .81). In addition to the inter-rater reliability, the persistence over time with the same case and information (whiting-rater concordance or test-retest reliability), and between-contexts concordance (estimating whether other encoders, equally trained, would get similar results) was analyzed (Monteiro, Vázquez, Seijo, & Arce, 2018). In this study, two researchers rated 30 CPVR each, then repeated their own assessment of three cases and did the rating of tree cases of the other researcher. Inter-rater and the intra-rater (test-retest) reliabilities were high (> .9) in both cases. At the same time, one of the researchers also showed reliability in its coding in a previous study (Loinaz, et al., 2017). Data Analysis Contingency tables (chi-square tests) and odds ratios were analyzed, comparing the prevalence of presence of each risk factor (“Yes” and “?” were added to facilitate 2 x 2 comparisons). To obtain a numerical risk level, risk factor codifications were translated to coding of 2 (Yes), 1(?), and 0 (No). This allowed a comparison of mean scores (t-test) between groups as well as use of the score for prediction purposes. Binary logistic regression analyses were conducted to identify best predictors of CPV group (clinical or judicial). All bivariate significant variables except psychopathology and presence of a CPV complaint were included. Psychopathology was not included because differences were considered to be possibly due to types of assessment conducted at each center, given that often, in clinical settings, one target is diagnosing pathology. CPV complaints (to police or in court) were not included because of their direct relation as a previous step in being attended to in a judicial context. The enter method and the backward stepwise method (with likelihood ratio method) were used, beginning with all bivariate significant variables and eliminating variables that did not contribute to the prediction model or were not significant. Following the significance of the Wald statistic (p < .005) and Exp(B) confidence interval (not including value 1), some predictors (2, 12, 18, and 22) were eliminated from successive analyses. Finally, ROC curve analyses were used to determine how well the tool distinguished the type of offender and the presence of injuries. Possible cut-off scores were calculated analyzing the area under the curve (AUC). Main Risk and Protective Factors Table 1 shows the comparison between the prevalence of risk and protective factors of both samples. The judicial sample showed more complex violence contexts with more bidirectionality and violence other than CPV, and greater rates of complaints filed for CPV. As to the psychological issues of the perpetrators, the only variable that was significantly more prevalent in the clinical group was the presence of psychopathological symptoms (including symptoms or diagnosis of disorders like conduct disorder, depression, and so on). For the other variables, there were either no differences between the two groups, or the risk factors were more prevalent in cases that were treated in legal contexts (empathy problems, anger management, narcissism, and attitudes justifying violence). Regarding variables of adaptation, there were significantly more antisocial relationships and more histories of failure in previous interventions in the judicial sample. The block of family factors was the one that demonstrated the most significant differences between groups. In all six variables of which it is composed, the prevalence was higher in the judicial context, suggesting more conflicts and personal problems of parents, problematic education style, and inversion of the hierarchy. The protective factors were, as a whole, more frequent in the clinical sample, confirming a better case profile for this group. Other Factors Included in the CPVR In Table 2 other risk factors present in the first section of the CPVR are compared. Judicial cases had significantly more single-parent families, and siblings who also had histories of aggression. In the judicial sample there was higher prevalence of parental criminal records (50.0% vs. 2.2%), higher prevalence of injuries to the mother (53.3% vs. 3.3%), and more than 40% of the group had histories of violence other than CPV (42.9% vs. 18.4%). On the other hand, only clinical cases saw offenders coming from adoptive families (21.3%) and in this sample as well there was longer duration of violence (6.3 vs. 3 years). The age of onset was earlier in the clinical group (M = 11.7, SD = 3.81) than in the judicial one (M = 13.2, SD = 2.51), although the difference was not statistically significant (p = .051). Table 2 Prevalence of Other Factors Included in the Tool 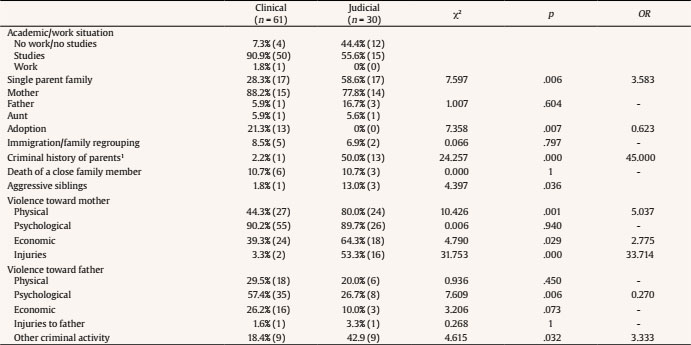 Note. 1Although the item includes both parents, in this sample only fathers had criminal records. Predictors and Classification After several logistic regression analyses, four variables (see Table 3) emerged with significant predictive power, with an accurate classification of 89.4% of all cases: narcissism, attitudes, violence between parents, and personal problems of parents. The prediction was better for clinical cases (94.8%) than for judicial cases (77.8%). Although bidirectionality was significant in some steps, prediction for judicial cases improved when this factor was eliminated from the model. Table 3 Binary Logistic Regression Results  Note. Model χ2(4) = 49.540, p = .000. Hosmer-Lemeshow = .750; Cox-Snell = .442; R2 Nagelkerke = .619. Quantitative Risk Assessment Taking a quantitative perspective, there was a difference in the total score of risk factors in the CPVR, which was significantly (p = .000) higher in the judicial sample (M = 25.86, SD = 8.51) than in the clinical one (M = 14.25, SD = 7.94). According to AUC value, total score distinguished the type of group (AUC = .830, 95% CI [.733, .926], p = .000), and the presence of injuries to mother (AUC = .764, 95% CI [.637, .891], p = .001) with a large effect size (Salgado, 2018). The best cut-off score for group classification and injuries to mothers was between scores of 22 and 23 as can be seen in Table 4. Paying attention to the Positive Predictive Value (PPV), adopting a cut-off score of ≥ 23, 69% of perpetrators classified as high risk were being attended to in a judicial context, and 83.9% of low risk offenders were being treated in a clinical context. If a cut-off score of ≥ 22 is adopted in regard to injuries to the mother, 41.9% of cases labeled as high risk saw injuries to the mother, while 91.7% of low risk cases did not. The PPV permits an answer to the following question: when a case is labeled as high risk, what is the probability that this case will be treated within a judicial context or will include injuries to the mother? On the other hand, the Negative Predictive Value (NPV) allows one to know the probability that a case labeled as low risk will be in a clinical system or will not have injuries to mother. For both results, the prediction was always more accurate for the negative case (being clinical or no injuries). Table 4 Cut-off Score Prediction of Group and Injuries to Mother  Note. TP = true positive; TN = true negative; FP = false positive; FN = false negative; Sens. = sensitive (true positive fraction) = TP/(TP+FN); Spec. = specificity (true negative fraction) = TN/ (TN+FP); PPV = positive predictive value = TP/(TP+FP); NPV = negative predictive value = TN/(TN+FN). The aim of this paper was to compare two samples of CPV offenders, coming from clinical and judicial contexts, according to risk and protective factors assessed with a new violence risk assessment tool, the Child-to-Parent Violence Risk assessment tool. We wanted to know what differentiates cases, leading to some being treated in private therapeutic contexts and others intervened upon by the judicial system. As far as we know, this is the first study comparing these types of cases. First, the type of violence was found to be different among groups, with more injuries to mothers in judicial cases, although physical violence to fathers was slightly higher among clinical cases, with earlier age of onset and longer duration of the abuse in this latter group. Taking this into account we can hypothesize, as will be discussed later on, that each group corresponds to a different type of CPV or reflects an evolution in offenses and type of situation from less to very severe. With regard to personal variables of offenders, diagnoses of psychopathology were more prevalent among clinical cases (mainly because the clinical diagnostic is often sought out in the clinical context), but psychological profiles were worse in the judicial group. Academic problems and antisocial behaviors were equally prevalent in both groups, but judicial offenders had more antisocial friends and failures in previous interventions. This pointed to the higher therapeutic needs of these children. Contreras & Cano (2015) compared CPV cases with those of other young offenders and non-offender adolescents, finding the highest presence of psychopathology and social-cognitive difficulties in the CPV group. We did not find significant differences among groups for drug abuse. Although the prevalence of this problem was lower compared to previous research, the result is also congruent with the finding that drug consumption is not a key variable to differentiate types of young offenders despite it being important in comparing non-offenders to offenders (Contreras & Cano, 2015). Impulsivity seems to be a common characteristic of CPV offenders and other young offenders (Contreras & Cano, 2015; Rico, Rosado, & Cantón-Cortés, 2017), and in our case both groups had the same high prevalence. Self-esteem also did not show differences, matching previous studies in which no differences in self-esteem were found either between CPV offenders and general offenders (Contreras & Cano, 2015; Ibabe et al., 2014a; Kennedy et al., 2010), or between CPV offenders and non-offenders (Ibabe et al., 2014b). Antisocial peers and failure in previous interventions were also more prevalent in judicial context. An aspect found repeatedly in previous research is the risk related to family factors. As expected, judicial cases had significantly higher prevalence in all risk factors related to family problems (i.e., problematic education style, conflicts, violence). Results of parental supervision and discipline are inconsistent (Ibabe & Bentler, 2016), but negligent parenting style (little support and little control) has been found to increase the probability of physical and verbal violence towards parents (Contreras & Cano, 2014b; Gamez-Guadix et al., 2012). Parenting style may be associated both with externalizing problems (i.e., authoritarian style) as well as good behavior (i.e., affection, communication) (Ruiz-Hernández, Moral-Zafra, Llor-Esteban, & Jiménez-Barbero, 2019). Single parent families were more prevalent among judicial cases. Previous research has found this prevalence to be higher among CPV cases compared to other offenders (Contreras & Cano, 2014a, 2014b; Ibabe & Jaureguizar, 2010), commonly with the mother in charge (Kethineni, 2004). It has been suggested that the increased risk of CPV against single-mothers may be due to other problems related to family organization or concomitants of divorce, and not only to being a single-parent or mother (Pagani, Larocque, Vitaro, & Tremblay, 2003). Moreover, violence committed by parents is a particular risk factor in CPV (Del Hoyo-Bilbao, Gámez-Guadix, & Calvete, 2018). Added to the higher prevalence of victimization by parents in the judicial context and related in the literature with a higher presence of physical and psychological aggression towards parents (Gámez-Guadix & Calvete, 2012), there were also more violent and non-violent conflicts between parents in the judicial sample. This bidirectionality has been described in a third of the cases referred to court, with judicial CPV offenders having been victims or witnesses in up to 80% of these cases (Ibabe et al., 2009). Parent-to-child violence has also been shown to be a consistent predictor of CPV in previous research (Gallego et al., 2019). This first finding was confirmed in our judicial sample (with it having been five times more probable to be a victim at home), and 50% of the full sample had been a victim or witness of violence (violence between parents was 11 times more probable among judicial cases). Exposure to different forms of family violence can explain between 16% and 45% of the aggressions of young people to their parents (Morán, González-Álvarez, & García-Vera, 2011) and, therefore, it should be an issue to consider in intervention and prevention programs. CPV cases are more likely to have histories of violence in the family (as victims or as witnesses) compared to general youth offenders (Contreras & Cano, 2014a). One explanation is that children’s behaviors may affect parenting behavior, and that continual aggressive behavior in adolescents may launch a negative cycle of family interactions (Contreras & Cano, 2015). Kethineni (2004) hypothesized that “juveniles could have modeled their own behavior on what their parents customarily did in conflict situations.” (p. 388). Finally, there was a higher prevalence of personal issues of parents of judicial CPV offenders. Previous research has pointed out that issues such as drug consumption in parents can lead to inconsistent communication of norms or enforcement of discipline (Pagani et al., 2009), and depressive symptoms may be related to psychological abuse, specifically for mothers (Ghanizadeh & Jafari, 2010). On the other hand, half the fathers of offenders in the judicial system had criminal records, compared to only 2% of fathers in clinical cases. Contreras & Cano (2014b) sugest that this risk factor is comon among CPV offenders and other youth offenders. The prevalence found in this judicial sample is similar to the 48.2% found by Kethineni (2004), though the current study did not replicate criminal records found for mothers in Kethineni’s study. Research on CPV and protective factors is scarce, and a recent study analyzing this used a type of protective factor not commonly used in risk assessment research (Beckmann et al., in press), namely, the opposite of some risk factors as protective factors (i.e., positive family relationship, high self control). Moreover, little is known about the utility of protective factors in other youth offender risk assessment tools or even results go in an unexpected direction. For instance, Hilterman, Nicholls, and van Nieuwenhuizen (2014) found that SAVRY’s protective factor total scores did not add incremental validity over SAVRY risk total scores. In our sample, groups differed on the prevalence of family involvement in therapy and children’s social support. While prevalence of family involvement was higher in clinical cases, social support was found to be greater in judicial cases. Family implication may be related to family functionality and cohesion, and it is considered by clinicians a predictor of good prognosis. The finding of greater social support among judicial cases is not easy to explain but may be related to the deterioration of family relationships, leading to more frequent interaction or help seeking outside the family. This tool has been shown to be useful in the classification of diferent types of CPV offenders (AUC = .830), and even to discriminate the presence of injuries toward the mother (AUC = .764). Moreover, cut-off scores were useful to correctly classify up to 79.1% of offenders into the correct group, and 74.7% of those with or without injuries to the mother. This study presents some limitations that should be taken into account to understand results and implications. First, there were more girls in the clinical sample, which may have biased the results. The sample was also not representative as far as it was small and not randomized. Moreover, the comparison was made between CPV offenders without a control group of non-offenders or other offenders who had not committed CPV. Future research could be more accurate by comparing more groups to analyze whether there is a progression in the risk profile or whether the different approach adopted in cases of CPV (i.e., legal or clinical) is truly chosen by the family or rather due to family type (i.e., differences in possibilities, resources, and so on). There were not scores for the different risk factors (i.e., psychological features), so comparison was only made in a categorical way (presence vs. absence). Having specific scores in some dimensions could help to better understand the differences found. Together with the practical implications for prevention and detection (detecting evolution of violence or managing the case according to risk level), some questions are derived from this research that should be addressed in future studies. First, prospective follow-ups to establish predictors of recidivism or treatment success will be needed. At the same time, the utility of protective factors should be addressed. Whether CPV is a type of domestic violence or a type of youth offense is another question. So far, studies looking at this specific comparison (Contreras & Cano, 2014a, 2014b, 2015; Ibabe et al., 2014b; Kennedy et al., 2010) have found some differences among types of offenders that we have found also within our samples. According to these and previous results, it seems that there may be a continuum or dimensional evolution in CPV cases, from more “normal” or less criminal, and more similar to non-offenders (i.e., our clinical sample), to more antisocial or criminal offenders, who are more similar to other youth offenders than to non-offender groups (i.e., our judicial sample). Another research line to be developed is to address the gender-specific relevance of the risk and protective factors, as has been done recently (Beckmann et al., in press; Del Hoyo-Bilbao, Gámez-Guadix, Orue, & Calvete, 2018; Rico et al., 2017), or to establish specific weighting for each risk factor to arrive to actuarial results, which could be useful for decision making of front line practitioners. This work shows the potential of the CPVR in daily practice when classifying cases within intervention programs or even assessing possible evolutions of cases. Its application in different contexts or with different predictive aims will strengthen its usefulness for clinicians and front line professionals. aConflict of Interest aThe authors of this article declare no conflict of interest. Cite this article as: Loinaz, I. & de Sousa, A. M. (2020). Assessing risk and protective factors in clinical and judicial child-to-parent violence cases. The European Journal of PsychologyApplied to Legal Context, 12, 43-51. https://doi.org/10.5093/ejpalc2020a5 References |
Cite this article as: Loinaz, I. and Sousa, A. M. D. (2019). Assessing Risk and Protective Factors in Clinical and Judicial Child-to-Parent Violence Cases. The European Journal of Psychology Applied to Legal Context, 12(1), 43 - 51. https://doi.org/10.5093/ejpalc2020a5
iloinaz@ub.edu Correspondence: iloinaz@ub.edu (I. Loinaz).Copyright © 2025. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License







